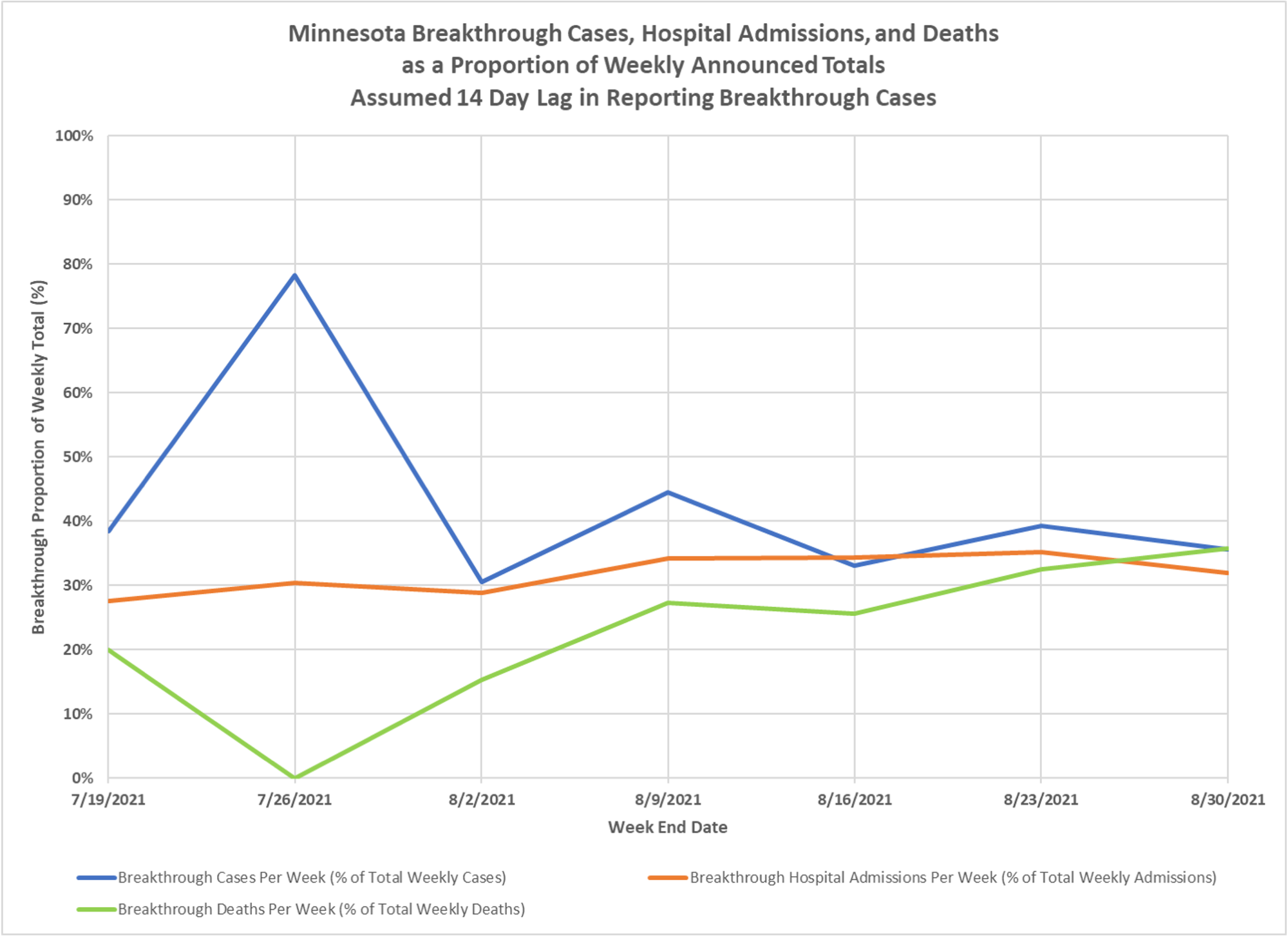
Breakthroughs are reported on Monday, hard to match them up with the appropriate time period on a date of event basis, but remaining at about 35% of all events, and the proportion of deaths is climbing. Thanks to Dave Dixon.
Breakthroughs are reported on Monday, hard to match them up with the appropriate time period on a date of event basis, but remaining at about 35% of all events, and the proportion of deaths is climbing. Thanks to Dave Dixon.

© 2026 Healthy Skeptic.
What to make of all this?
What is the expected level of “breakthrough deaths”?
I find it hard to square 35% level of “breakthrough death” with 95% vaccine effectiveness.
So, if the lines were to reach around 50% and hold steady there, it would mean that being vaccinated and not being vaccinated are of equal efficacy?
no, depends on the relative size of the groups. There are way more vaxed people than unvaxed in Minnesota at this point.
Yes Kevin, I am also trying to square the vaccines continued protection against severity but rapidly waning protection against infection. What’s the immunology here?
Does a 35% breakthrough death rate, which is increasing over time, indicate the vaccinations were massively oversold? I think it does.
Let’s run through some basic math which I think even I am capable of, and see what it tells us.
Starting at this Minnesota website the claim is, as of today, 93.2% of the population 65+ and 73% of the population 16+ got the shots: https://mn.gov/covid19/vaccine/data/index.jsp
– Let BRD be the breakthrough death rate. I assume it is defined as number of vaccinated people who died “of COVID” divided by total number of people who died “of COVID” in the period.
– Let POPVR be the population vaccination rate. It is defined as number of people in the population who got two vaccine doses divided by the total population.
Then the ratio R = BRD/POPVR tells us how effective the vaccine is at preventing death “from COVID”. If R = 0, the vaccine is 100% effective. If R = 1, the vaccine is 0% effective. If R > 1, the vaccine is causing people to die “of COVID”.
Taking those Minnesota government numbers, we see that the overall population rate of 73% translates into R = 0.35/0.73 = 0.48. This means that in an equal size population of vaccinated and unvaccinated people, 48 vaccinated people die “of COVID” for ever 100 unvaccinated people who die “of COVID”. To me that says the vaccine is only 52% effective at preventing death (it prevented 52 out of 100 possible deaths).
That’s FAR CRY from what was promised, and if as we have strong reason to suspect, the number is going down over time, it could get worse.
Note that if you use the 93% 65+ vaccinated number it still only translates into 62% effectiveness at preventing death, which is sill FAR CRY from what we were promised, and the 93% assumption is way too generous because we know people under 65 are dying. And we also know about the sleight of hand where single dose people get counted as unvaccinated.
Is my math wrong? If so, show me how. And not just how it is wrong but how doing the math right transforms into significantly better performance.
But to me these numbers are devastating. Especially since I thought prevention of hospitalization and death is what these vaccines were supposed to be good at.
I don’t think your math is right, you set up the problem wrong
Who pays for Flu vaccinations of ?50% of the population every year? Is it your medical plan, I’ve seen “Free” signs around at times. I’ve never gotten one, so I just don’t know. According to what’s available to research, this new virus displaced the Flu viruses. Or, we’ve been dealing with a combination of Covid and Flu, but calling it all Covid based on the fraudulent PCR scheme and the need to market and amplify the political fear factors.
How is big pharma going to make their earnings without a Flu vaccine production run this year … unless they have a new boogie man called Covid to replace it?
I was under the impression that the definition of an effective vaccine was 50% protection for 1 year … under this definition, it’s a looser. But hell, definitions and medical terminology today are up for grabs depending on the illusion and message you want to send.
https://www.aier.org/article/uncle-sams-hamartia-your-early-death/
To my point !
I don’t mind being:
(A) shown the error of my ways;
(B) shown how the error can be corrected; and
(C) shown how the corrected approach translates into a substantial difference in the analysis.
But I’m not super interested in being told I’m wrong without any backup.
—-
For further clarity the purpose of the arithmetic, it is to “scale” the breakthrough death rate to match the population vaccination rate, so that people stop making the claim that “high breakthrough death is fine, because the vaccinated population is just so much higher that it doesn’t matter”. Instead of relying on that claim without numbers, let’s quantity what the difference is, and what that difference really tells us about the vaccines.
—
By the way, Moderna has finally come out and admitted that their vaccine performance weakens over time: https://nypost.com/2021/09/15/moderna-says-new-data-supports-need-for-booster-shot/
charts coming tomorrow. Among other things the analysis should be done by age group and the analysis should compare the truly non-adaptive immune, from vax or infection, with the vaxed.
Looking forward to the chart!
Agreed that the age structure is useful for the more nuanced picture. However, if the point of that is just going to be that “all the breakthrough deaths are in old people and that’s fine because old people are vulnerable”, well, I’m not convinced. After all, ALMOST ALL COVID deaths are also in old people. None of the fomented panic that pushed us into the clown world we are in now would even have succeeded if it weren’t for the fact that you had 70+ people with one foot already in the grave dying in high numbers. Those old weak vulnerable people are the very people whom the vaccine should be protecting if the vaccine is rationally connected to the actual cause of the panic.
I disagree with the second point. Why should people who have immunity from prior infection and haven’t received a vaccine be subtracted from the unvaccinated column, thus artificially depressing the results? If that is being done, the people who ALREADY HAD immunity from prior infection and still got the vaccine should be removed from the vaccinated column, because they are very likely to be artificially improving the vaccine’s claimed effectiveness. Because they already had immunity.
The adjustments should get us closer to the truth, even if the truth is the vaccines are a slow motion train wreck that is only just getting started.
If you are trying to demonstrate the effectiveness of a vaccine intervention in protecting people without adaptive immunity, you can’t include the infected. Otherwise what are you suggesting, the appropriate intervention to protect people from infection is to get them infected?
YES !!
I think it’s arguable that the NET health and wellness effects of letting the Alpha virus run through the US population, with normal and proper medical intervention as early as possible and isolation of the the sick, would have resulted in far less death and destruction to the society as a whole. I believe it was called the Leicester Method. Here’s one article, there are many others.
For purely political reasons, there’s been hyper focus on a medical issue that has a 99% survival rate with lies about the numbers at every opportunity for purposes of distortion. Now people are trying to apply mathematics, charts and graphs to explain compounded lies and phony data. In business as in life, your first loss is your smallest. The more you stir a pile of SH*T, the worse it smells.
https://vaxopedia.org/2017/05/06/the-leicester-method-and-smallpox-eradication/
I tend to agree with J.Thomas, but that was not my point.
My point is, as YOU have written, millions upon millions have already been infected, survived, and earned their adaptive immunity. If you EXCLUDE these people from the unvaccinated category, you are exaggerating the magnitude of the problem to be solved, and likewise exaggerating the benefit of your solution (“vaccines”).
This is because the unvaccinated but immune population will tend to reduce the relative benefit of the vaccine.
You create a narrative that vaccines are, to be charitable, 75% effective in the “unvaccinated” because you have excluded those unvaccinated people who tend to improve the standing of the unvaccinated group.
This approach is only valid in a world that recognizes immunity from prior infection, but we are not in that world, we are in clown world. And in clown world, to quote your president, “the unvaccinated are a risk to the vaccinated”, and that is that. Needles for everyone, do not ask any questions.
Even if we somehow exit clown world, what do you say about the other half? Anyone who has immunity from prior infection should be excluded from the “vaccinated” group even if vaccinated. Otherwise you are exaggerating the effectiveness of the vaccine by allowing it to arrogate the effectiveness of the person’s existing immunity.
Also, to simplify with an expression I recently learned, what’s sauce for the goose is sauce for the gander.
you don’t want to be vaccinated fine, but admit that that is completely coloring anything you say about the vaccines. That level of feeling should be a warning to you that it is highly unlikely you are thinking rationally on the topic.