Here is the actual chart from the paper I mentioned in the earlier post. You can see that even among the elderly, the vaccine is effective against serious disease. Adjustments are important to understand what you are actually seeing.
Here is the actual chart from the paper I mentioned in the earlier post. You can see that even among the elderly, the vaccine is effective against serious disease. Adjustments are important to understand what you are actually seeing.

© 2026 Healthy Skeptic.
Hey Kev, wondering about risk versus reward. I’m over 50 and not vaccinated. Using the Israeli data, I have a one-in-a-thousand chance of getting a severe case of Covid and an even smaller chance of dying from it, which doesn’t seem like bad enough odds to justify taking much risk with the vaccine. I read elsewhere that Israelis had a bunch of severe reactions to the vaccine but can’t seem to find data on it.
Do you have data to perform a risk-of-reaction-to-vaccine versus risk-of-severe-Covid-case analysis?
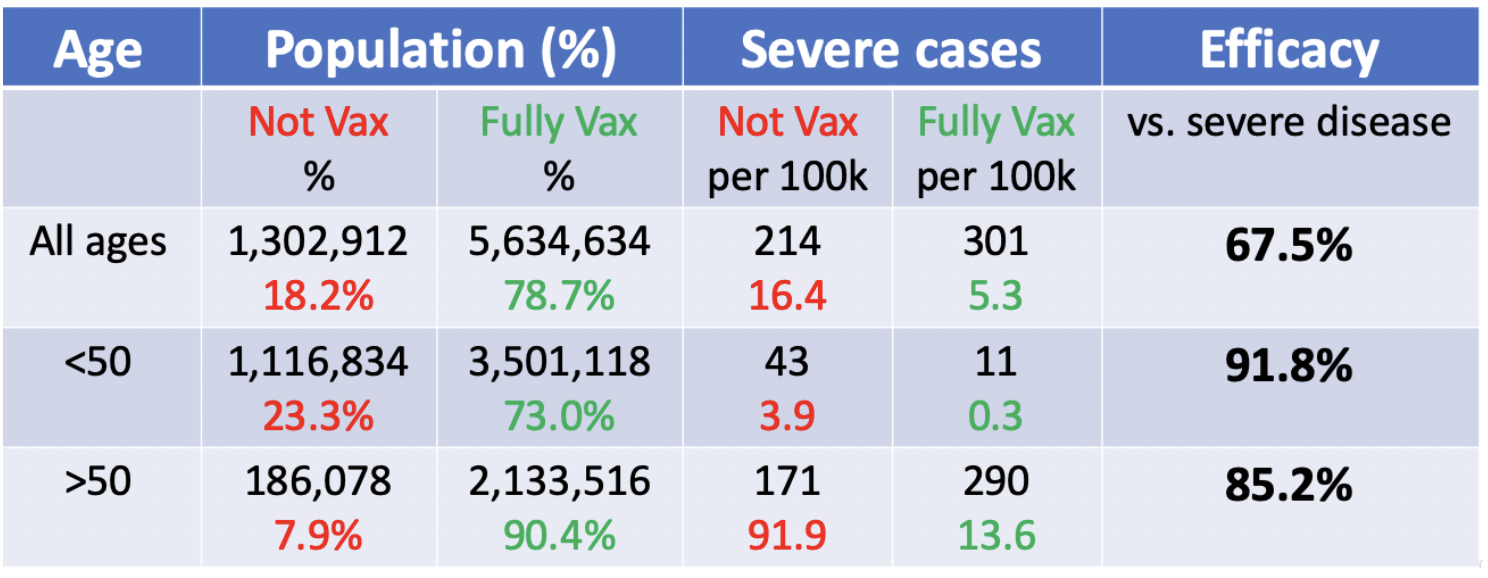
Am understanding this chart right?
The figures are given “per 100K population” so we should be able to compare the figures without reference to the underlying vaccination rate.
Let’s agree beforehand that the majority of the at-risk population is over 50. Therefore we are most interested in the >50 row of the table.
What I see is for over 50, unvaccinated have 171 severe cases per 100K and vaccinated have 290 per 100K, or roughly 60% more severe cases in the vaccinated cohort.
Am I missing something? Help me understand how this table provides evidence of the vaccines’ efficacy for older people, and not the opposite. Was there some context in the earlier post that makes these figures make sense?
the color coding is throwing you off, those are the cases, not the rate
Thanks so much for your blogs, which I just recently found when you were mentioned in Powerline. Excellent work and well referenced. You are on top of the key CV issues. Thanks to you I found Jeffrey Morris’ blogs, so lots of good reading there for me to catch up on, too.
I have a few Qs.
1. How is is established when a positive CV test is due to delta variant (DV)? My understanding is that DNA sequencing is needed to distinguish DV. Here in HI it is claimed that 90-95% of our current “cases” are DV, but the state capacity to do sequencing is 50-100 samples/wk. Is CV prevalence guesswork or extrapolation? Is there a DV-specific quick assay?
2. Given that the 60% of those vaccinated have completed their final shots ranging from weeks to 7-8/mo ago & those already infected that are “breakthrough” range form perhaps 3-16/mo previously infected…….How can these differing lag periods and current CV Ab levels be accurately compared?
3. Are the breakthrough infections attributable to DV primarily? If so, what value would a booster have if designed vs the original CV strain vs the current range to newly emerging variants?
4. In terms of those previously infected with CV and then receiving one of the vaccines….are these any restudies or evidence that they are more protected from breakthrough cases……and, does this group of infected+immunized have any increase in adverse reactions to the vaccine?
5. Did you weigh in the lab leak vs. animal origin issue? Given the 2-3 yrs+ work In Wuhan funded my Dasik and work from Barik messing with CV genetics and testing in cell & animal models……you would think it would be very important to get detailed info on the Spike protein and other CV functional features to get info regarding emerging CV variants and what we should mot be worried about. Although the original aim of GoF research was vaccine development……now this lab & experimental info could be put to good use in the current pandemic setting. Why no interest from the CDC and NIH? Wouldn’t Moderna and Pfizer like to see the unpublished Wuhan and Baric work to provide insights into future vaccine formulations? I just don’t get it. I was 15yrs in biomed research with a PhD. We were trained to be curious, ask Qs, and seek out threads of knowledge leading to new information. Biomed research in 2021 is all science fiction + political science. Plus, researchers that know the truth can’t speak out.
Yes, it’s kind of sad the people like Berenson that are always on TC misrepresent the Israel vaccine data. But, this is just what you get with the MSM…even from those you like best…..Berenson was at least useful in fighting masks and lockdowns. The best you can trust anything you see in TV is 50% (at best), even TC often falls below this level, sadly.
What’s the date range data was collected? Or did I miss it?
It was in the study and I probably forgot to include it. It ran to pretty recently as I recall.
The article says through August 15