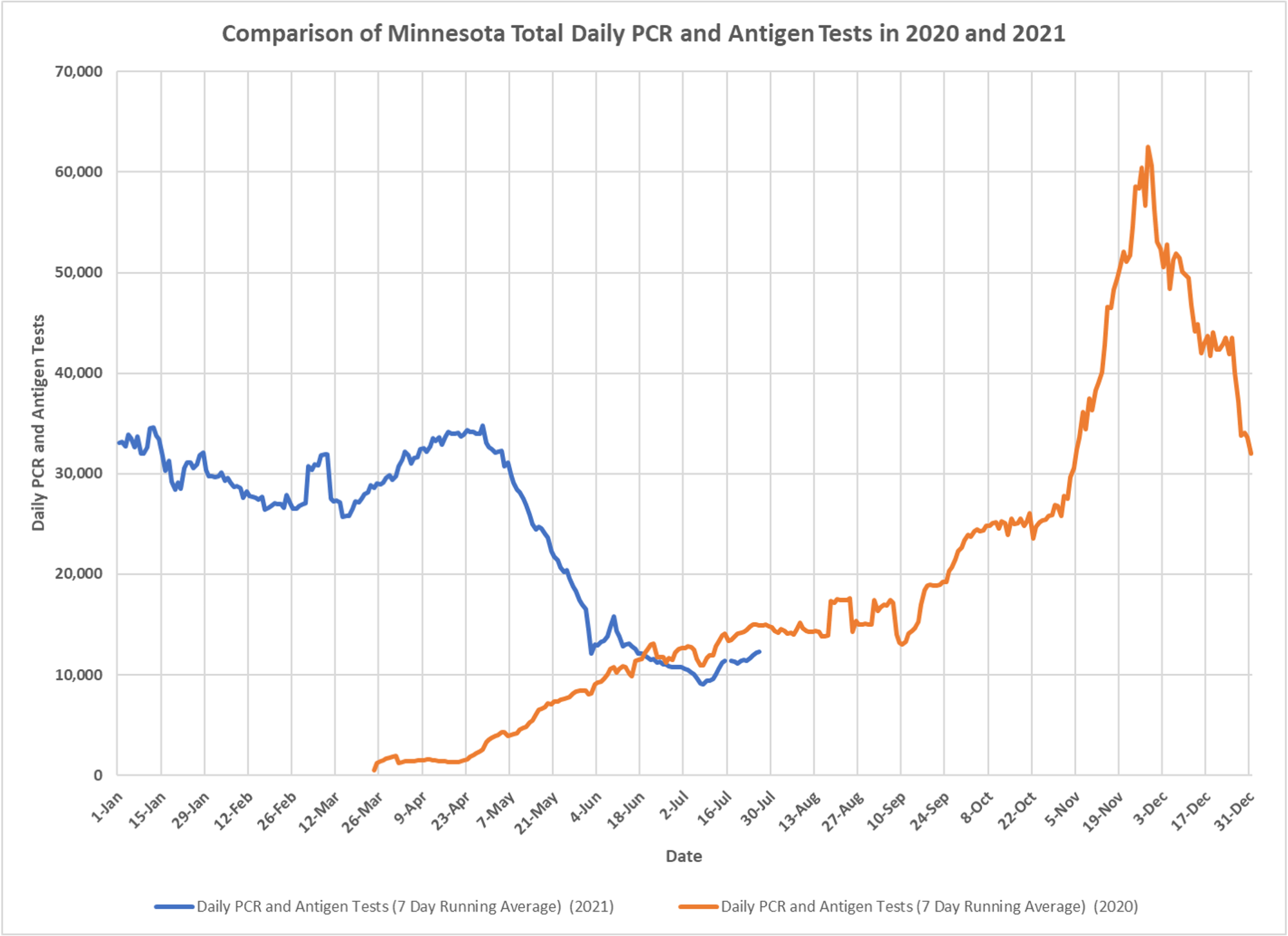
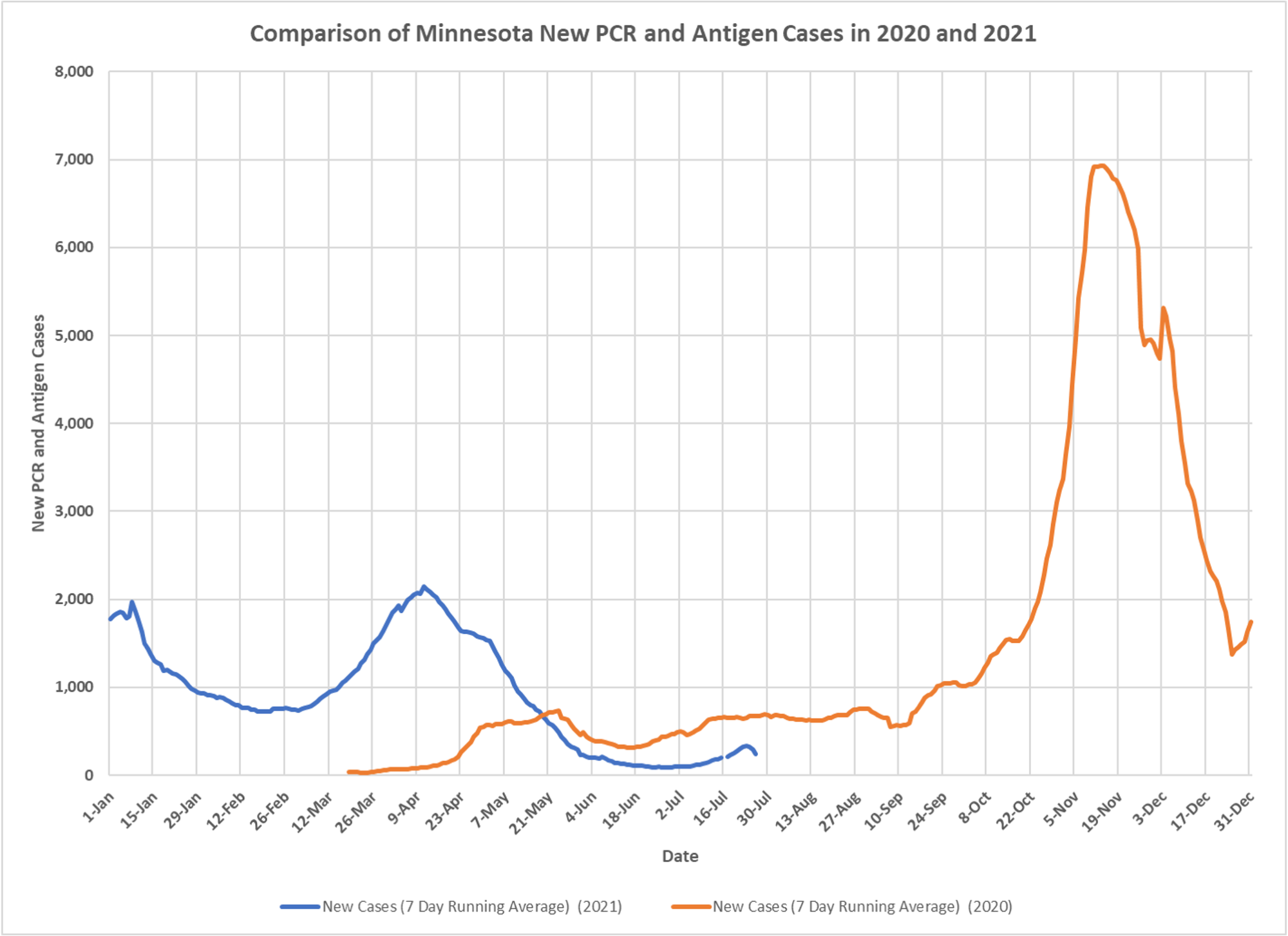
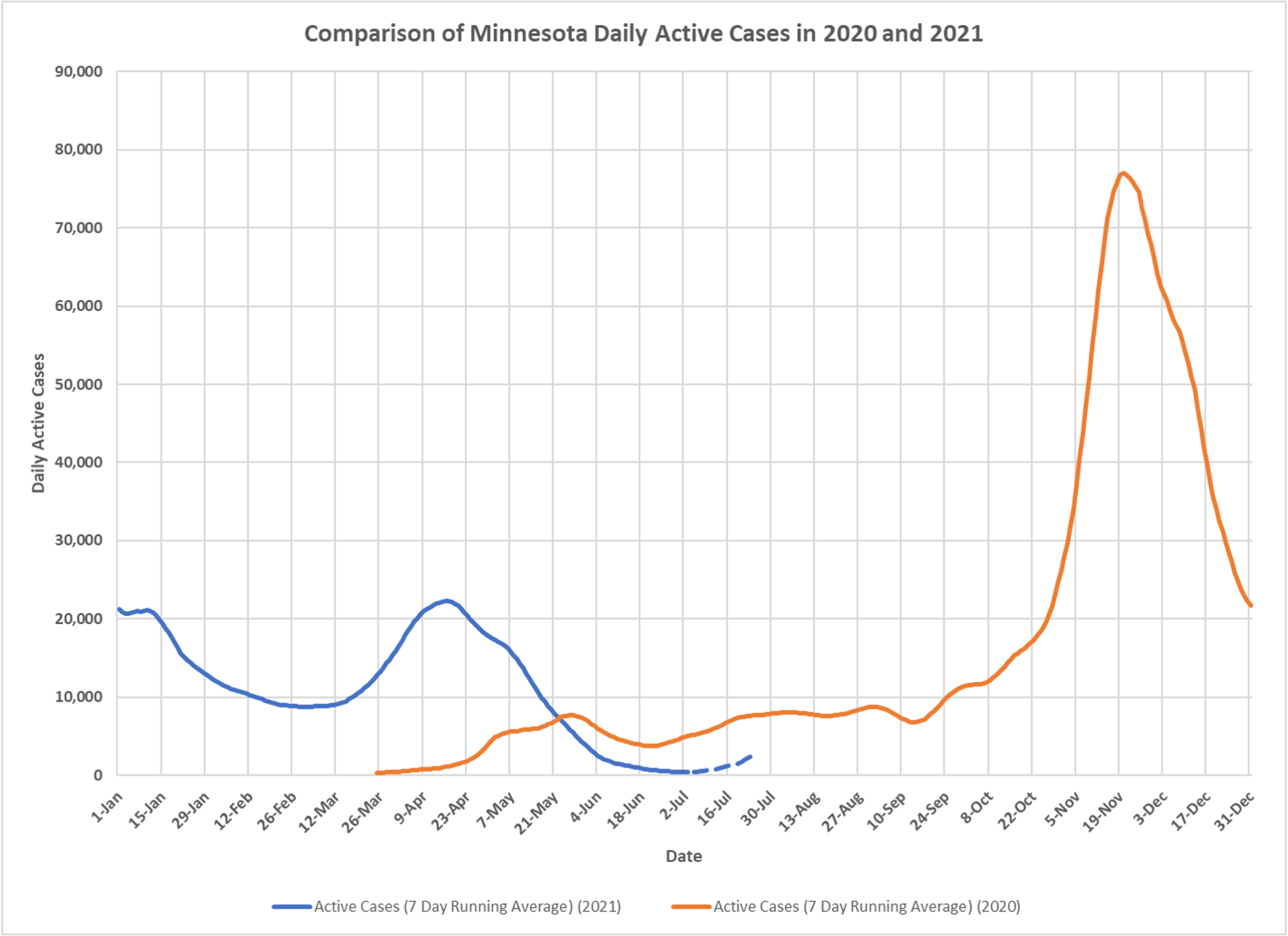
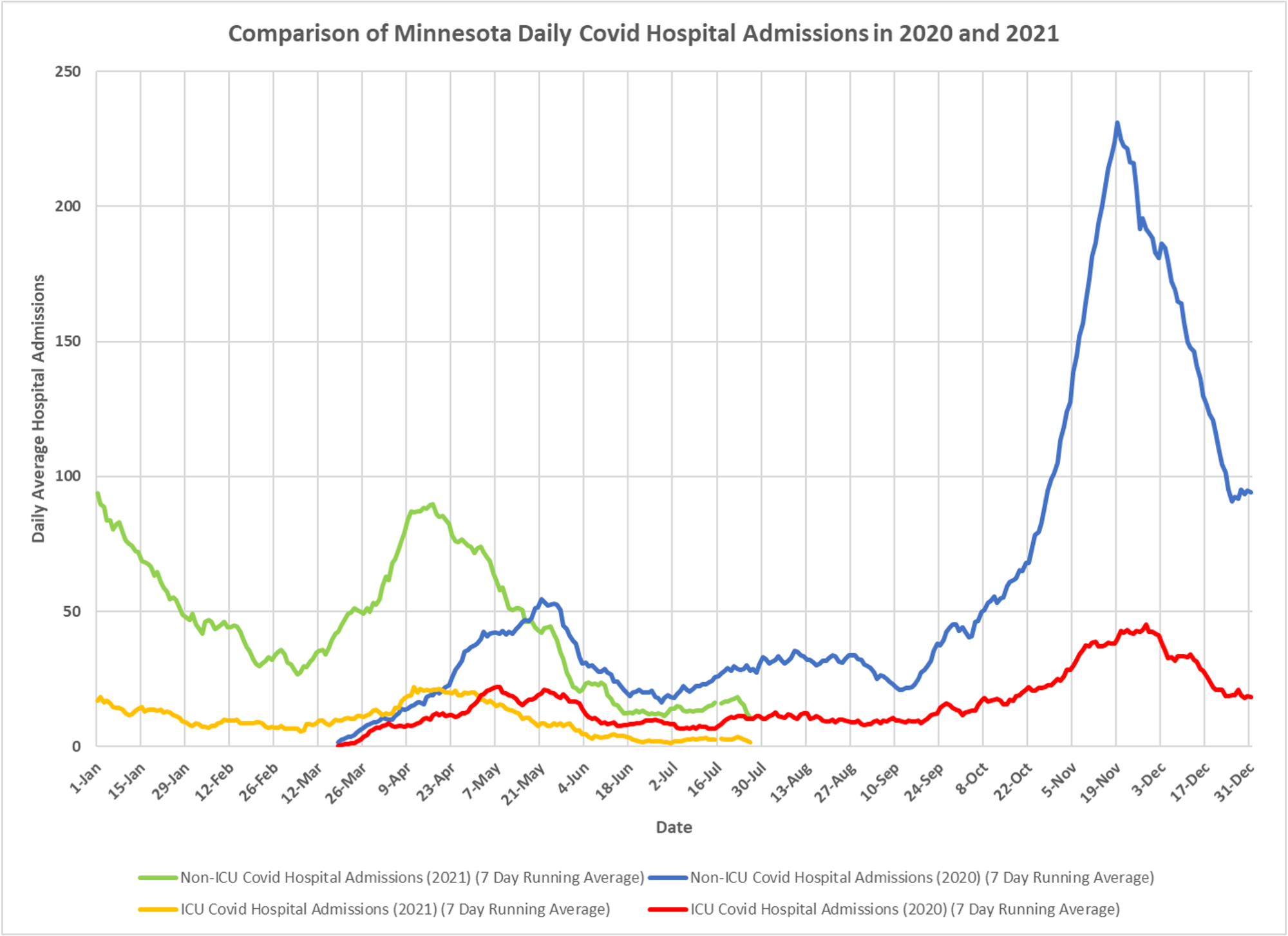
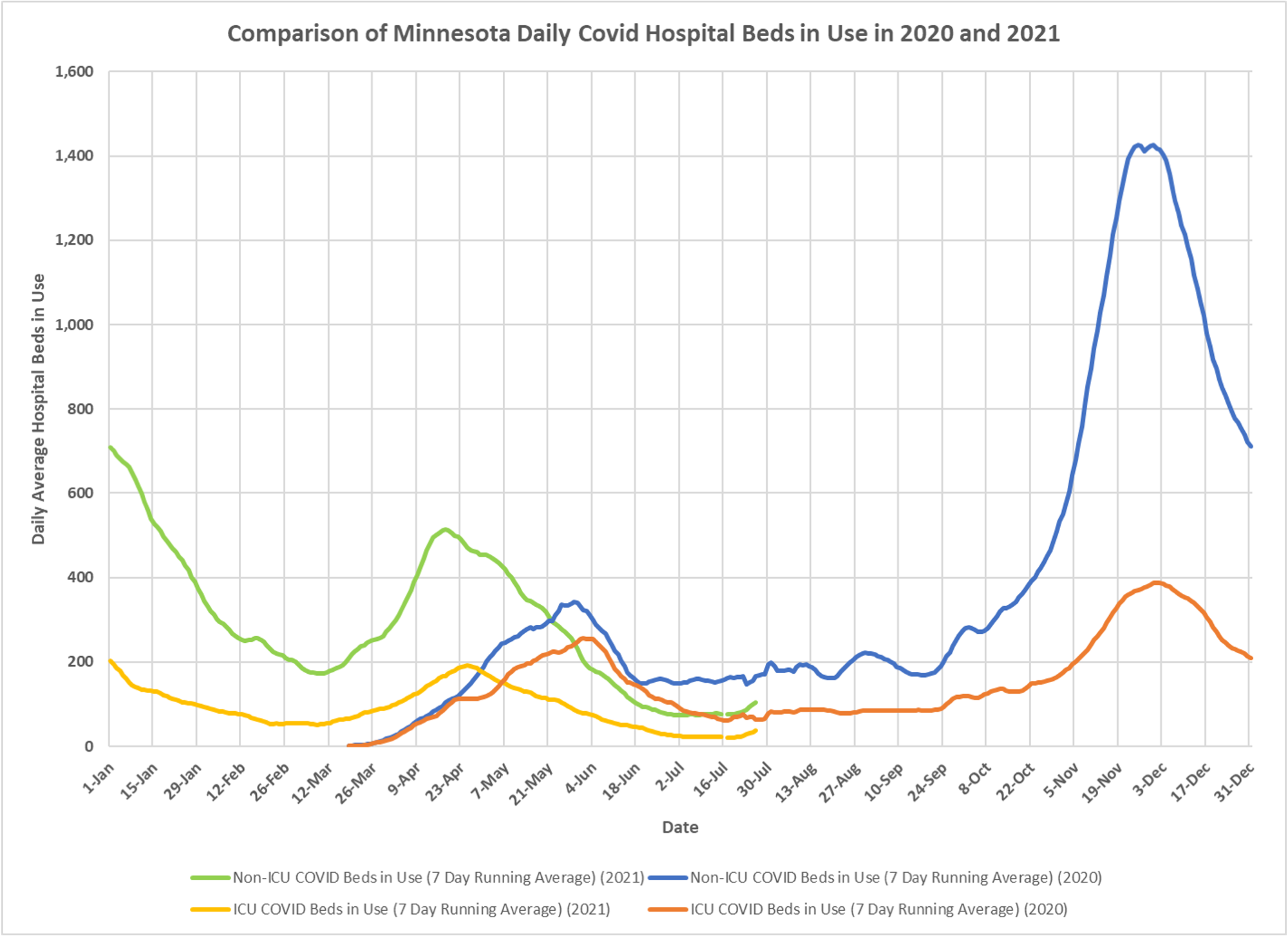
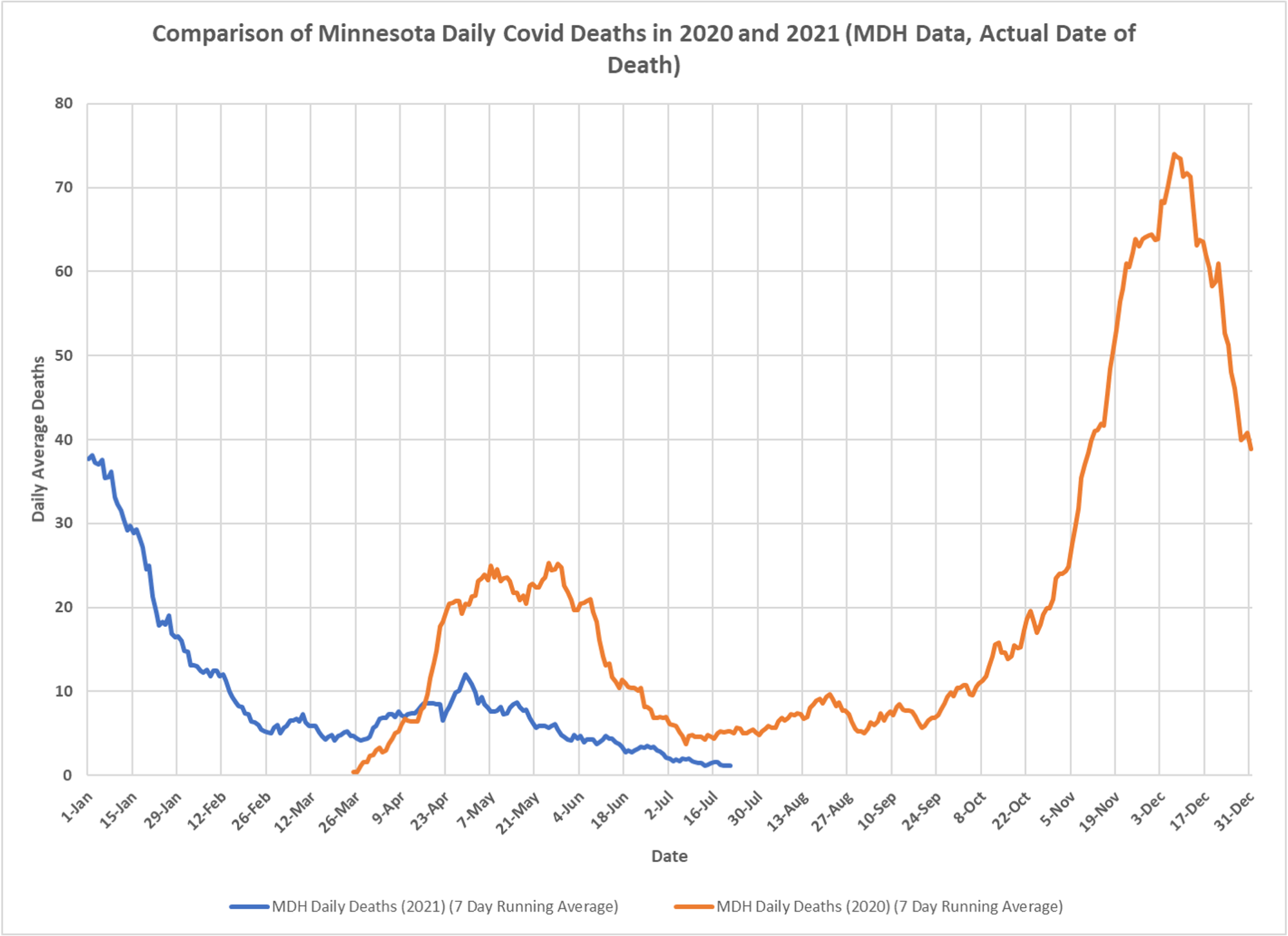
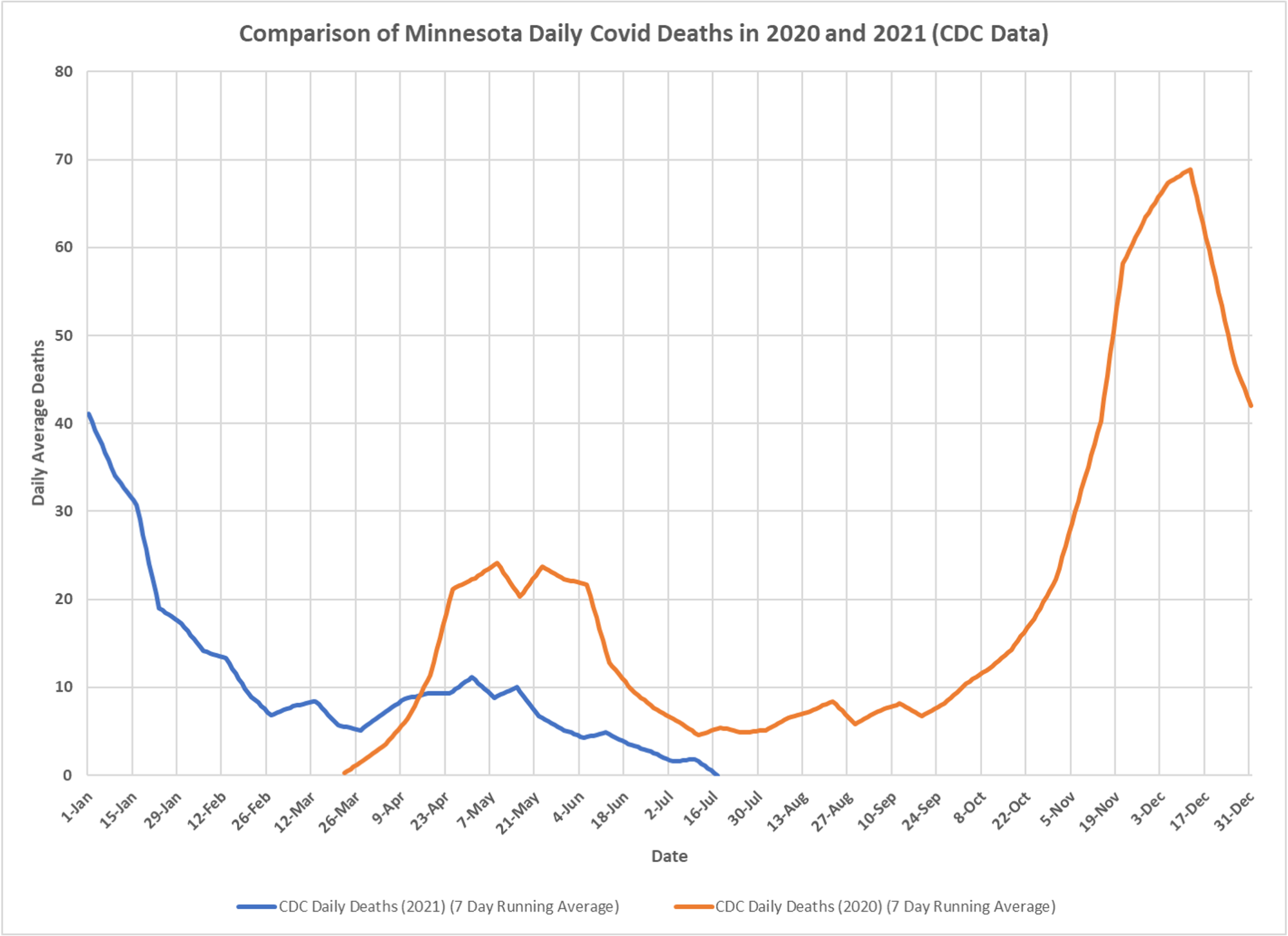
For those of you tempted to believe Alex Berenson’s and others’ drivel about vaccines not working, look at these charts from Minnesota. Even though testing is at similar levels now, cases are down, hospitalizations are down, deaths are down. Adaptive immunity at work. Thanks to DD.

I’ve been reading Alex Berenson’s “drivel” on Substack trying to assess whom to agree with (between Kevin, Alex, and others). One observation about these Minnesota charts is that if I understand correctly they aren’t addressing the substance of the “drivel” head on. Alex is writing about Israel and the UK, different countries with different “vaccination” velocities, “vaccine” mixes, and ultimately different data. My understanding is the US charts do look quite different from the Israel/UK charts at the same point in time. As well, some types of apples-to-apples comparisons are made more difficult because the US data are less transparent.
Kevin, one thing that would lend your writing more heft is to make a direct frontal assault on one of Alex’s arguments and show, specifically, where the flaw is. Otherwise a lot of the writing just looks like borderline ad hominem about “drivel”, “terrorism”, etc. Clear writing focused on the point is a major source of credibility to those few of us who still aim to read, understand, and be persuaded by reason, rather than just swallowing packaged conclusions we are already predisposed to believe.
Another credibility booster would be stop being so obsessive about the “vaccines” and the USA. There is a bigger world out there. Countries such as India and continents such as Africa have had totally different experiences to the USA. Sweden has achieved zero COVID deaths week over week. Cheap, safe, drugs such as Ivermectin are in use in various places with clamed success. To only speak about America and highly profitable Big Pharma products smacks of shilling for the pharmaceutical industry or being afraid to speak about topics out of fear of censorship. At least grapple with these countries, regions, and therapies and explain why they are such bad options that it is preferable to make every healthy person in the world into a beta tester of a brand new “vaccine” with no long term data, and which just happens to make lots of money for large corporations. Otherwise the relentless focus on “vaccines” seems disingenuous, to say the least.
My focus is the US and to some extent Minnesota, I reference global studies or events in other countries when they may be enlightening here. I am not going to spend time with deep analysis in other places and I don’t understand what that has to do with pharma companies or therapeutics. Alex Berenson is statistically illiterate, and hops around using whatever country he thinks he can twist to make his point. You may have noticed he isn’t talking about the UK anymore, doesn’t fit the message. The UK has turned down sharply in cases and never had a death uptick, I posted charts showing that. And we now know that hospitalizations in the UK have been greatly overstated although they were lower anyway in this wave. Alex also does things like refer to anyone who thinks the vaccines have effectiveness as a vaccine “fanatic”. he consistently misled about adverse event data, and you may notice he is off that kick as well, just didn’t pan out. I don’t know what his problem is about vaccines, but misinformation really riles me because it supports the crowd that thinks we should just lockdown and mask forever.
In regard to Israel, the data that has been published by their researchers shows high vaccine effectiveness. Alex references supposed official data which is incomplete in terms of age structure, per capita rates, cycle numbers, serious outcomes, etc. It is hard to do the same thing I can do with UK data when I don’t have access to that. I have no reason to think that the virus or the vaccine acts significantly differently in different countries, so when I look at actual research or at data from places with more complete elements, I tend to think that is more likely to reflect reality. I do think seasonality plays a role in any case bump, we see that in the year-over-year charts, particularly in the US. If someone has a better explanation than vaccine effectiveness and natural adaptive immunity for why rates of serious illness are so low in the US, I would be interested to hear it.
Similarly in the US, we have the lowest per capita mortality rates for the entire epidemic, certainly true also in Minnesota. I post charts several times a week demonstrating that year-over-year and just by absolute numbers, we are seeing lower rates of deaths and hospitalizations. Cases are tricky because of issues with PCR tests. I have also spelled out very specifically what additional information is needed to do even better analyses of what is actually happening. But what data would anyone point to in Minnesota to say vaccines aren’t working? The cases and the case rise are clearly almost exclusively among the unvaxed.
Kevin, thanks for your patient answer. I appreciate your willingness to explain things, sometimes over and over again. Your points about Alex are well made and I’ll pay better attention to, for example, bait-and-switching around UK data and the some of the other concerns you raised.
Agreed that calling someone a vaccine “fanatic” is typically unhelpful, though truth be told there are many real fanatics out there – Emmanuel Macron being just one example. I don’t see you as a “fanatic”, and I read this blog because you seem to present the research results pretty even-handedly. However, I would argue the blog’s significant focus on vaccines and vaccine effectiveness isn’t the most productive way to stop the insanity, if it can ever be stopped at this point. I’d love to hear your research opinion on Ivermectin, the overall India approach, the Sweden approach, etc.
Here are some reasons why I want to hear about other things than vaccines:
1. A sceptic, and a healthy one, should consider all the alternatives even if only to reject them.
2. Where’s the emergency? Eighteen months or so ago, the public health commissars used media-driven hysteria and the pretext of an emergency to seize unprecedented control of daily life in most parts of the developed world. Whether there was ever an emergency is debatable, but if there was one it has by now surely passed. Yet a sizable part of the population is continually “looking past the sale” (the emergency) and just accepting the premise that these “temporary” powers are now more or less permanent. Now that vaccine status shaming and second class citizenship for unvaccinated people are normalized, with outright vaccine administration by force just around the corner in some countries, I fear that focusing on vaccine effectiveness is playing into their hands. Compliance emboldens them; and it empowers them in each new round of goalpost shifting. We need to undermine the state of fake emergency. We need to publicize any alternatives, if they exist, and question why the authorities ignore them. If Ivermectin is effective both as a prophylactic and therapeutic, as claimed, the argument that any state of emergency exists is vaporized, in my opinion. And why would I ever beta test a drug for which no long-term side effect data exist? If it is ineffective, should we not know so as to look focus our attention elsewhere? If the data are mixed on Ivermectin, what do we need to know to decide?
3. I will soon have to choose between losing my job and “voluntarily” receiving a drug I do not need or want. The obsession with vaccines feeds the normalization of othering the unvaccinated population. It emboldens not only the commissars who work for the “real” government but also those who work for the corporations which in fact govern huge parts of the lives of hundreds of millions, if not billions. (And to be frank I don’t believe “just until everyone is vaccinated” any more than I believed “just until we flatten the curve”. There’s always a new way to control us.)
4. In general, if the Swedish model worked in terms of producing herd immunity with no worse health outcomes than countries and regions which went with hard lockdowns and hard vaccine pushes, what possible justification could there be for these steps?
This blog is a public treasure, and I thank you for writing it. If you have time, would you consider giving some thoughts on some of these other topics, including especially Ivermectin and why it should be ignored in favour of purchasing products from Big Pharma.
Well said, Abhijit.
It seems to me the vast majority of mainstream media discussions on these topics have a myopic focus on lockdowns, testing, masks, and vaccines, as if only these topics merit attention. Assessment and debate of preventive and/or early treatment options is little or missing, be that about ivermectin, vitamin d levels, role of obesity, etc.
I am sorry about the situation your employer has created. FWIW…
https://vivabarneslaw.locals.com/upost/889925/vaccine-mandate-protest-letter