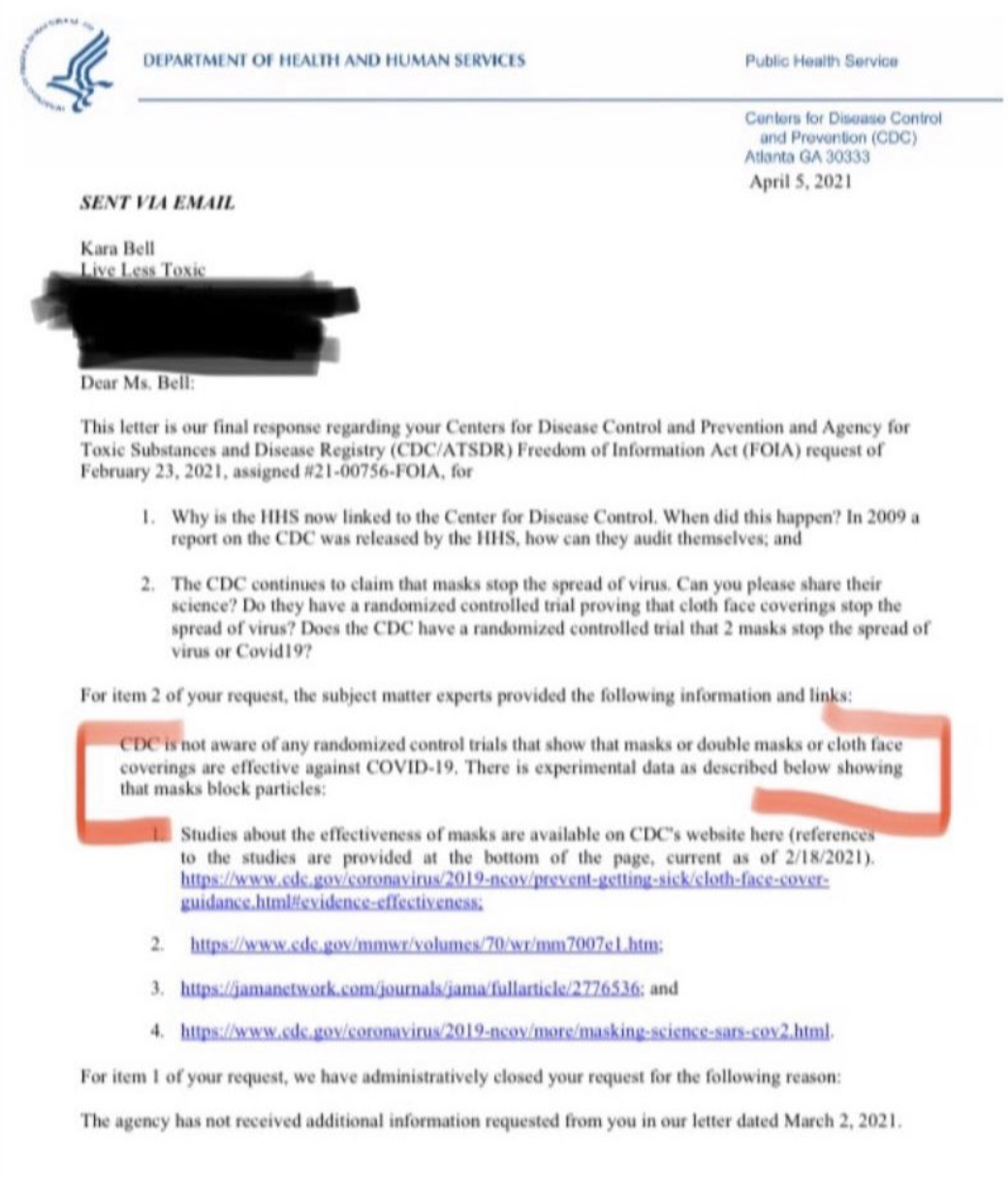
Freedom of Information Acts are wonderful things. Someone went after the CDC to provide data supporting mask mandates and policies. The responsive letter is below. Note the acknowledgment that there are not randomized control trials that support efficacy of masks. They note only some research that says masks block particles, and even that is sketchy.

This is a great recent document to use for my anti-mask forays here in un-scientific San Francisco. We still have ~90% outdoor mask use! Good job by Kara Bell. Thanks Kevin.
As a biochemist, getting results in vitro which do not translate in vivo is the story of my life. This is my take on why masks may work in the laboratory but not in the general population, why RCT studies of influenza and Covid19 usually show the masked group has slightly (but not significantly) lower infections than the unmasked group.
1) Most people will not spread the virus. The vast majority of people are either uninfected (cannot spread) or asymptomatic (rarely spread). If spread is low and the effect is small, then statistically it is hard to show significance even if the effect is real. Far more likely is that masks do work – but mainly for people who sick or people who get close to those who are sick (especially if the person who is sick has tuberculosis – see below). So only the sick people should wear masks or those who are close to them.
2) If people are physically distancing and therefore far enough away that they do not spread the disease, masks cannot have any effect. You cannot reduce the chances of getting CoVid to less than zero.
3) Human behavior? Do people who wear masks physically distance less?
4) Mask mandates and masks are two different things (apples vs. oranges). One reason a mask mandate may not work is that they do not increase (or increase only slightly) the number of people wearing masks.
5) We know most CoVid is spread in private settings, parties and at home, places where I’m willing to bet that even people in the masked groups seldom wear masks.
6) I don’t know about you, but it seems to me that a large proportion of my breath goes above, below and around the mask.
Masks were designed to protect patients from liquid-born droplets of bacteria falling from the top of a surgeon’s gastrointestinal track (i.e., her mouth), not air-borne viruses.
Thoughtful post, SteveD—a good read to start my weekend! All of your points are good food for thought. I have spent too much time this past year looking into mask research—my two cents are below. I have not included links to specific research; however, here is a link to a blog post by Bad Cattitude on Substack. This person went by @boriquagato until their account was banned on Twitter. This person appears to be a gem and the blog format gives them a more complex platform than Twitter.
https://boriquagato.substack.com/p/cdc-admits-no-rcts-support-mask-efficacy/comments
1. Yes, the fear of asymptotic spread has contributed greatly to mask mania. I point to the letter in the New England Journal of Medicine in spring 2020 which stated an asymptotic woman from China infected business contacts in Germany. It turned out she was on over the counter medication to mask her symptoms. The correction to the letter never received the publicity the original conclusion did.
2. Distance is a factor, yet exposure time may also be a component of spread. I haven’t found anything that explains spread risk by component. I did see a small study which showed healthcare workers contracting COVID from patients even while wearing n95 masks and face shields.
3. Strong point here—and precisely echoes your observation of results in a lab versus results in real life.
4. Exactly.
5. I think that is a dirty (not so little) secret of all the contact tracing that’s been done. And as you rightly point out, it’s doubtful a meaningful number of people will mask up at home. Furthermore, I’ve been surprised at the attack rate of infections in homes—for how transmissible we’ve been told this virus is, I would have thought anyone who lives with an infected person would automatically get sick. But that is far from the case.
6. This speaks to aerosol transmission and it’s what I keep going back to. Why can’t otherwise intelligent people understand that if a significant portion of spread is through aerosols, cloth masks are virtually useless?
And your final paragraph raises an excellent point. In researching mask use for viruses, I’ve found what appears to be strong evidence that mask use in an operating theater has no correlation with incidence of wound infection in the patients. Of course, I imagine it will take a lot more than a couple of studies to change the medical profession’s operating room procedures. Then again, if the patient feels safer because the surgical team is masked up, what does it matter that they are useless?
The procedures aren’t based on science they are based on lawsuits.
‘exposure time may also be a component of spread.’
That is likely true Darin. It made me recall another point I thought of a while back.
7) There is likely a (narrow?) range of a combination of factors including, physical distance, duration of contact, viral load, humidity, air circulation, size and type of virus or bacteria, etc. within which, masks have a chance to limit infection but beyond which they are useless. For example, a long and close contact with someone shedding a high viral load might overwhelm the mask making it ineffective, but a short contact with an asymptomatic has very little chance to infect, and therefore the mask is ineffective in that case also. In between there might be a sweet point where the masks can operate with some degree of effectiveness.
‘strong evidence that mask use in an operating theater has no correlation with incidence of wound infection in the patients.’
‘Then again, if the patient feels safer because the surgical team is masked up, what does it matter that they are useless?’
Maybe the masks are redundant with the other precautions which would not make them completely useless, but this might be a case where the additional precaution is justified for those rare cases where the mask might make a difference. It’s probably far easier for the doctor to infect the patient via his hands than his mouth.